https://medicalxpress.com/news/2021-01-vaccine-wars-escalate-antibody-variants.html

Credit: Wikipedia
With the rapid identification of these new variants within the infected population, and also in lab-generated versions of the spike protein, an exhaustive escape variant matrix has begun to take shape. The good news is that as long as the actual antibody responses of vaccinated individuals are tested and verified, the individual's response to different variants can, at least in theory, be predicted. The full response of our innate and adaptive immune systems to a fragment of a key viral entry protein will never be exactly the same as the response to natural infection with whole live virus, but in terms of generating similar antibodies that target key epitopes, it is often good enough.
The bad news is that efforts to thwart infection can, in some cases, inadvertently contribute to selection of more infectious variants. At least that is what researchers have concluded from their recent studies of new escape variants. To find out if antibody-imposed selection pressure could also drive the emergence of more infectious mutants, the researchers used an in vitro recombinant pseudotyped virus assembled from parts of the vesicular stomatitis virus (VSV) and also SARS-CoV-2. This avoids the hazards of working with full blown SARS-CoV-2, but retains the essential spike configuration. They found that every antibody they looked at selected for mutations in the RBD. Many of them selected for escape mutations identical to those now being seen in different locales, namely the E484, N501 and K417N variants. Individuals with suboptimal or waning immunity would therefore likely erode the effectiveness of natural and vaccine-elicited immunity.
While this may be a little disconcerting, the researchers suggest that antibody therapies should ideally be composed of combinations of antibodies that target non-overlapping epitopes. This may be challenging because the most potent and abundant human neutralizing monoclonal antibodies generated against SARS-CoV-2 (Class I and II antibodies) all seem to target residues near K417, E484 and N501. Half of the most potent antibodies found carried a heavy chain encoded by just one particular gene, IgHV3-53. The majority of these were more than 10 times less effective against pseudotyped viruses carrying the E484K mutation.
The researchers found that mRNA from vaccines encoding the spike RBD is translated to build spike fragments that generate antibodies very similar to those made by the real virus. Consistent with fully assembled spike protein trimers, the translated spike fragments spike showed proper adoption of the two expected states: the "up" state representing a receptor-accessible conformer and "down," representing a receptor-inaccessible conformer. In a further show of confidence, different individuals immunized with either the Moderna (mRNA-1273) or Pfizer199 BioNTech (BNT162b2) vaccines produced nearly identical antibodies.
In another recent paper, researchers generated a comprehensive map of nearly all (3804 of 3819) possible RBD amino acid variants for the early isolate Wuhan-Hu-1 version of the virus. They then tested them against recombinant antibody therapies including Regeneron's REGN-COV2 cocktail and Eli Lilly's LY-CoV016. They identified mutations that are selected in a persistently infected patient treated with REGN-COV2, as well as during in vitro viral escape selections, and one mutation, (E406W) that seemed to escape everything. Some of the identified escape mutations are already found in currently circulating SARS-CoV-2 strains.
None of these revelations have gone unnoticed by the big manufacturers. In fact, it gives them an opportunity to throw shade on their competitors, something that many are already doing now.
The bad news is that efforts to thwart infection can, in some cases, inadvertently contribute to selection of more infectious variants. At least that is what researchers have concluded from their recent studies of new escape variants. To find out if antibody-imposed selection pressure could also drive the emergence of more infectious mutants, the researchers used an in vitro recombinant pseudotyped virus assembled from parts of the vesicular stomatitis virus (VSV) and also SARS-CoV-2. This avoids the hazards of working with full blown SARS-CoV-2, but retains the essential spike configuration. They found that every antibody they looked at selected for mutations in the RBD. Many of them selected for escape mutations identical to those now being seen in different locales, namely the E484, N501 and K417N variants. Individuals with suboptimal or waning immunity would therefore likely erode the effectiveness of natural and vaccine-elicited immunity.
While this may be a little disconcerting, the researchers suggest that antibody therapies should ideally be composed of combinations of antibodies that target non-overlapping epitopes. This may be challenging because the most potent and abundant human neutralizing monoclonal antibodies generated against SARS-CoV-2 (Class I and II antibodies) all seem to target residues near K417, E484 and N501. Half of the most potent antibodies found carried a heavy chain encoded by just one particular gene, IgHV3-53. The majority of these were more than 10 times less effective against pseudotyped viruses carrying the E484K mutation.
The researchers found that mRNA from vaccines encoding the spike RBD is translated to build spike fragments that generate antibodies very similar to those made by the real virus. Consistent with fully assembled spike protein trimers, the translated spike fragments spike showed proper adoption of the two expected states: the "up" state representing a receptor-accessible conformer and "down," representing a receptor-inaccessible conformer. In a further show of confidence, different individuals immunized with either the Moderna (mRNA-1273) or Pfizer199 BioNTech (BNT162b2) vaccines produced nearly identical antibodies.
In another recent paper, researchers generated a comprehensive map of nearly all (3804 of 3819) possible RBD amino acid variants for the early isolate Wuhan-Hu-1 version of the virus. They then tested them against recombinant antibody therapies including Regeneron's REGN-COV2 cocktail and Eli Lilly's LY-CoV016. They identified mutations that are selected in a persistently infected patient treated with REGN-COV2, as well as during in vitro viral escape selections, and one mutation, (E406W) that seemed to escape everything. Some of the identified escape mutations are already found in currently circulating SARS-CoV-2 strains.
None of these revelations have gone unnoticed by the big manufacturers. In fact, it gives them an opportunity to throw shade on their competitors, something that many are already doing now.
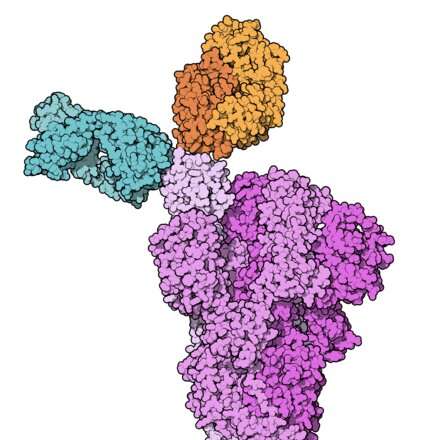
REGN10933 (blue) and REGN10987 (orange) bound to SARS-CoV-2 spike protein (pink). From PDB: 6VSB, 6XDG.
Credit: Wikipedia
The New York Times reported Monday that officials in the Phillippines have now balked at the safety and efficacy of the Chinese Sinovac vaccine because of lack of any real data. In response, Chinese state media has started a campaign against the American vaccines, questioning the safety of the Pfizer and Moderna shots and distributed online videos.
Over in the EU, the vaccine race has also turned ugly with the German government now publicly questioning the efficacy of the Oxford/AstraZeneca vaccine. In a highly disputed release, they called the vaccine "85% effective on older people." The EU has also threatened to block exports of the Pfizer vaccine to Britain. Many of the criticisms being levied have centered on the question of whether or not the vaccines may be the cause when people, particularly older people, die a short time after they are vaccinated. No reasonable person is saying that vaccines can never sicken or even kill susceptible people, and no reasonable person is saying that all vaccinated people who die did so because of the vaccine they just had. The patent animosity between two very different vaccine ideologies, i.e., "vaccines can do no harm" vs. "all vaccines are evil," is unproductive for everyone.
If SARS vaccines are safe and effective, then we all need to know that, because presently, a game-changing fraction of the population is simply not going to accept rapidly deployed vaccines. On the other hand, if these new vaccines are a danger to a minor portion of people who are immunologically susceptible to their effects, then we need to find out who is at risk ahead of time. The first step forward is for both sides of the argument simply to recognize that on the one hand, control of the immune system through vaccines is perhaps our greatest and most coveted technological capability, and on the other, that in the current state of advancement, incompletely understood vaccines are fallible for a non-negligible, yet still incompletely known, portion of the populace.
In many present cases, informed, yet conflicting opinions are all we have. For example, when someone everybody knows dies, like home-run champion Hank Aaron, and he also happened to have a vaccine 15 days earlier, some people are going to ask questions. Questions are neither bad, nor wrong; they are questions. If the cause of death is unknown, and no one can point to obvious preconditions or apparent symptoms consistent with possible vaccine injury, then the only facts available are the times of death and time of the vaccine. Therefore, no worthwhile truths or conclusions can be immediately drawn.
On the other hand, when someone dies 16 days after a vaccine, like Miami obstetrician Gregory Michael, and a cause of death is later determined to be something that is known to cause problems with other vaccines like MMR, and furthermore, is also considered a significant complication associated with SARS-CoV-2 infection, then more questions do need to be asked. In this particular case, the patient showed clear signs of immune or idiopathic thrombocytopenic purpura (ITP) three days after the shot, as he suddenly became riddled with numerous petechiae (dots) all over his body that indicated internal bleeding. Ultimately he died after suffering a hemorrhagic stroke, presumably due to the inability to muster sufficient platelets. When you live a half-century without petechiae, but get them when you inject a potential petechiae-causing agent into your blood, statistically speaking, you likely have more than correlation.
The problem is that when the manufacturer of the vaccine is put in charge of the investigation, and doctors from prestigious medical institutions across the country dismiss the case as a fluke, then people that have read the details of what happened to this man are going to push back and make it even harder for new vaccines to be accepted. If the narrative that establishment vaccine manufacturers are trying to convey is that Dr. Michael had a preexisting precondition to ITP, then people with the same condition need to be diagnosed before subjecting themselves to vaccines. For those few, vaccination is simply not worth the risk.
For vaccines to defeat a shapeshifting virus that evolves to the very vaccine itself, and not injure susceptible folks in the process, escape variant matrices need to be populated and genetic tests for known risk polymorphisms need to be done. We need to know what kinds of antibodies people make in response to the spike protein, whether they can block escape variant spike proteins, and whether they have pre-existing genetic disposition to vaccine injury like ITP. A tall, but necessary order if we are to banish this virus.

Recommend this post and follow The birth of modern Man
https://disqus.com/home/forum/lifeofearth/
No comments:
Post a Comment
Stick to the subject, NO religion, or Party politics